Article by Dr. Piyawat POOMSUWAN
A Scarring Hair Loss Disorder That Can Permanently Destroy Hair Follicles
Many people first notice that their forehead appears wider, their frontal hairline is slowly receding, or their eyebrows are becoming thinner. Some may also experience scalp burning, itching, or tenderness. These symptoms are often mistaken for “normal hair thinning” or age-related hair loss.
However, in some individuals, these changes may represent a condition called Frontal Fibrosing Alopecia (FFA) — a form of scarring alopecia that has been increasingly recognized worldwide over the past decade.
The most important fact about FFA is this:
If diagnosed too late, the hair follicles may be permanently destroyed and unable to regrow.
What is Frontal Fibrosing Alopecia (FFA)?
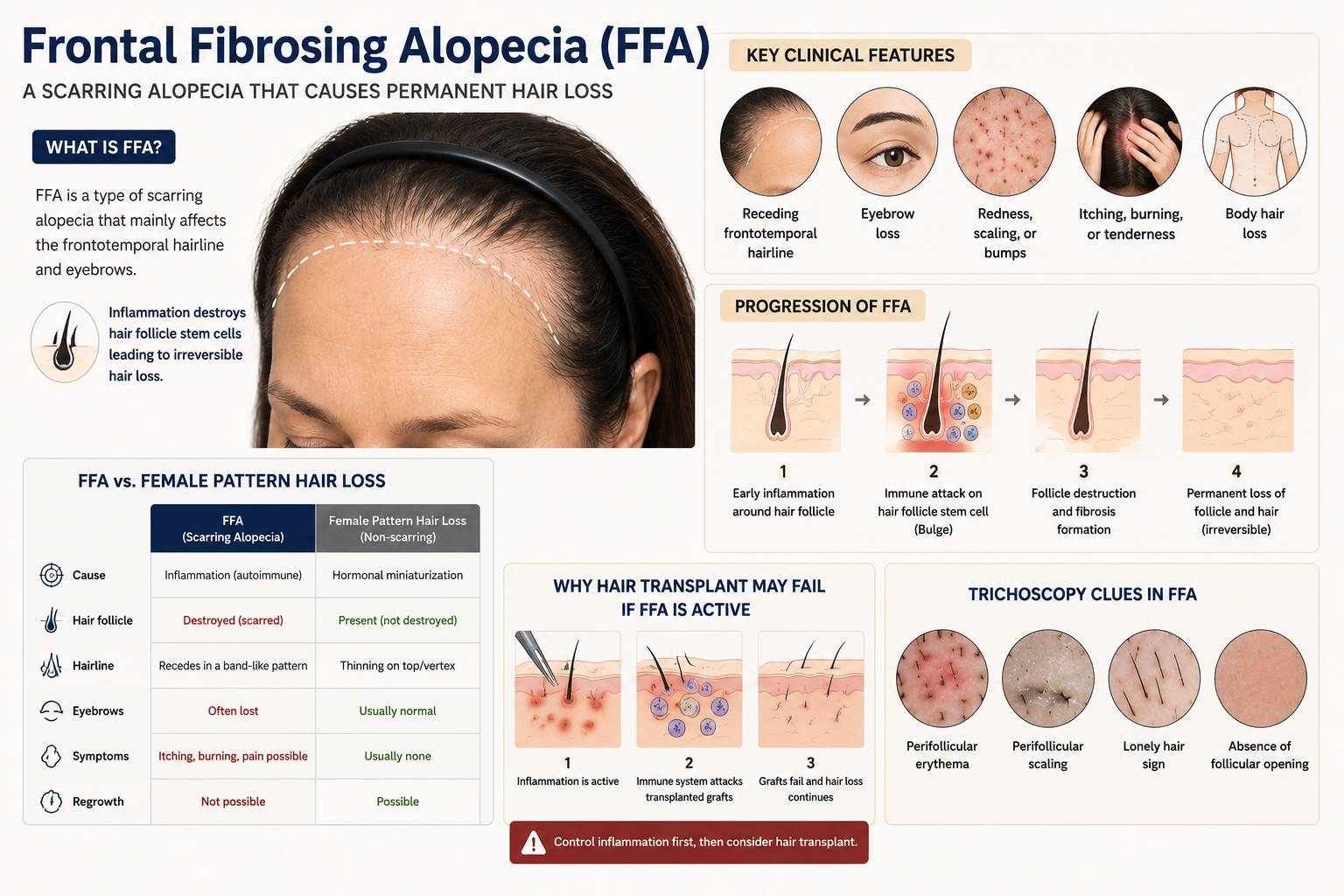
Frontal Fibrosing Alopecia (FFA) is a type of primary cicatricial alopecia (scarring alopecia) in which the immune system attacks critical structures within the hair follicle, particularly the region known as the hair follicle bulge, where hair follicle stem cells reside.
When these stem cells are damaged, the follicle loses its regenerative capacity, leading to:
- permanent follicle destruction,
- fibrosis (scar tissue formation),
- irreversible hair loss.
FFA was first described in 1994 and was initially thought to affect mainly postmenopausal women. However, it is now increasingly recognized in:
- premenopausal women,
- men,
- and younger individuals.
Many dermatologists worldwide have observed a significant rise in the number of FFA cases over the last 10–15 years.
What Type of Scarring Alopecia is FFA?
Scarring alopecia refers to a group of inflammatory hair disorders in which hair follicles are permanently destroyed.
Unlike common hair thinning disorders where follicles remain alive but produce thinner hairs, FFA causes:
- inflammation around the follicle,
- perifollicular fibrosis,
- destruction of sebaceous glands,
- replacement of follicles by scar tissue.
As the disease progresses, follicular openings may disappear completely, leaving smooth, shiny skin without the ability to regrow hair.
FFA most commonly affects:
- the frontal hairline,
- temporal scalp,
- and sideburn areas.
Additional findings may include:
- eyebrow loss,
- body hair loss,
- facial papules,
- scalp itching, burning, or pain.
How is FFA Different from Typical Hair Thinning?
FFA is frequently misdiagnosed as female pattern hair loss or androgenetic alopecia. However, they are fundamentally different conditions.
| Feature | FFA | Female Pattern Hair Loss |
| Main mechanism | Autoimmune inflammatory destruction | Hormonal follicular miniaturization |
| Follicle destruction | Permanent | Usually reversible in early stages |
| Hairline pattern | Band-like frontal recession | Diffuse thinning over crown/vertex |
| Eyebrow loss | Common | Uncommon |
| Scalp symptoms | Burning, itching, tenderness possible | Usually absent |
| Fibrosis/scarring | Present | Absent |
| Hair transplant outcome | May fail if disease is active | Often more successful |
Some patients may have both FFA and androgenetic alopecia simultaneously, making diagnosis more challenging.
Why Can Hair Transplant Surgery Fail in FFA?
One of the most important clinical concerns in FFA is that some patients undergo hair transplantation before the disease is properly diagnosed.
If inflammation remains active:
- the immune system may attack transplanted grafts,
- fibrosis may develop around newly transplanted follicles,
- transplanted hairs may fail to survive,
- progressive hairline recession may continue despite surgery.
In some cases, surgical procedures themselves may trigger disease activation through inflammatory mechanisms.
For this reason, patients with:
- unusual frontal hairline recession,
- eyebrow thinning,
- scalp redness,
- perifollicular scaling,
- or scalp burning symptoms
should be carefully evaluated for scarring alopecia before considering hair transplantation.
How Does FFA Progress?
FFA usually progresses slowly but continuously.
Many patients initially develop:
- eyebrow thinning,
- subtle frontal hairline recession,
- scalp discomfort.
Over time, progression may involve:
- widening forehead appearance,
- temporal recession,
- diffuse scalp involvement,
- body hair loss,
- facial papules.
One of the major challenges is that microscopic inflammation may continue even before visible hair loss becomes obvious.
Therefore, disease activity may still be present even when the scalp appears clinically stable.
What is “Irreversible Follicle Destruction”?
The hallmark of FFA is permanent destruction of the hair follicle stem cell region, particularly the hair follicle bulge.
This structure is essential for:
- follicle regeneration,
- hair cycling,
- and new hair production.
Once these stem cells are destroyed:
- the follicle cannot regenerate,
- scar tissue replaces the follicle,
- permanent hair loss occurs.
This is what makes FFA fundamentally different from ordinary hair thinning disorders.
What Causes FFA?
The exact cause of FFA remains unknown, but several mechanisms are believed to contribute:
1. Autoimmune Mechanisms
Immune-mediated attack against hair follicle stem cells is considered central to disease development.
2. Hormonal Factors
FFA is more common in postmenopausal women and may be associated with androgen metabolism.
3. Genetic Susceptibility
Familial cases of FFA have been reported, suggesting a genetic predisposition.
4. Environmental Triggers
Researchers have investigated possible associations with:
- sunscreens,
- cosmetic products,
- topical allergens,
- environmental toxins.
However, these relationships remain controversial and are not yet definitively proven.
Symptoms That May Suggest FFA
Patients should consider medical evaluation if they notice:
- progressive frontal hairline recession,
- widening forehead appearance,
- eyebrow thinning or loss,
- scalp burning or itching,
- smooth shiny skin without visible follicular openings,
- redness or scaling around hair follicles.
How is FFA Diagnosed?
Diagnosis is typically based on:
- clinical examination,
- patient history,
- trichoscopy,
- and sometimes scalp biopsy.
Trichoscopy often reveals characteristic findings such as:
- perifollicular erythema,
- perifollicular scaling,
- absence of follicular openings,
- lonely hair sign.
These findings help differentiate FFA from common non-scarring hair loss disorders.
Conclusion
Frontal Fibrosing Alopecia (FFA) is a form of scarring alopecia characterized by immune-mediated destruction of hair follicles, particularly the stem cell-rich bulge area.
Key points include:
- early symptoms may begin with eyebrow loss or subtle frontal recession,
- FFA is often mistaken for ordinary hair thinning,
- delayed diagnosis may result in irreversible follicle destruction,
- early recognition and disease control are critically important.
Today, FFA is increasingly recognized worldwide and remains an active area of dermatologic research involving immunology, genetics, hormones, fibrosis, and environmental factors.
References
- Kossard S. Postmenopausal frontal fibrosing alopecia: scarring alopecia in a pattern distribution. Arch Dermatol. 1994;130:770–774.
- Alenezi S, Ezzat RZ, Miteva M. Frontal fibrosing alopecia part I – Diagnosis and clinical presentation. J Am Acad Dermatol. 2026;94:1059–1072.
- Ezzat RZ, Alenezi S, Miteva M. Frontal fibrosing alopecia part II: Etiopathogenesis and management. J Am Acad Dermatol. 2026;94:1075–1085.
- Tziotzios C, Stefanato CM, Fenton DA, Simpson MA, McGrath JA. Frontal fibrosing alopecia: reflections and hypotheses on aetiology and pathogenesis. Exp Dermatol. 2016;25:847–852.
- Porriño-Bustamante ML, Fernández-Pugnaire MA, Arias-Santiago S. Frontal Fibrosing Alopecia: A Review. J Clin Med. 2021;10:1805.
- Kępińska K, Jałowska M, Bowszyc-Dmochowska M. Frontal Fibrosing Alopecia – a review and a practical guide for clinicians. Ann Agric Environ Med. 2022;29(2):169–184.
- Photiou L, Nixon RL, Tam M, Green J, Yip L. An update of the pathogenesis of frontal fibrosing alopecia: What does the current evidence tell us? Australas J Dermatol. 2019;60:99–104.
- Doche I, Wilcox GL, Ericson M, Valente NS, Romiti R, McAdams BD, Hordinsky MK. Evidence for neurogenic inflammation in lichen planopilaris and frontal fibrosing alopecia pathogenic mechanism. Exp Dermatol. 2020;29:282–285.
- MacDonald A, Clark C, Holmes S. Frontal fibrosing alopecia: A review of 60 cases. J Am Acad Dermatol. 2012;67:955–961.